
Transforming Smiles. Changing Lives
Experience the difference of concierge-level dental care in Corsicana, TX.
Meet Dr. Wright
For over 20 years, Dr. Wright has been the trusted choice for families across Navarro County and the greater Dallas–Fort Worth area. With deep roots in family dentistry and a passion for life-changing results, Dr. Wright specializes in smile transformations — including dental implants, All-on-4 restorations, and custom dentures. Decades of experience, a gentle touch, and a personalized approach that puts every patient at ease.
Voted a top All-on-X, full mouth dental implants provider in Texas.
Advanced surgical training and cutting edge same-day technology.
Gentle, honest, pressure and judgement-free care that puts you first.
Meet Dr. Wright
Voted Top Dental Implant Provider in Texas
Voted a top All-on-X, full mouth dental implants provider in Texas.
Advanced surgical training and cutting edge same-day technology.
Gentle, honest, pressure and judgement-free care that puts you first.
The Power of Advanced Medicine
Lorem ipsum dolor sit amet, consectetuer adipiscing elit. Aenean commodo ligula eget dolor. Aenean massa. Cum sociis natoque penatibus et magnis dis parturient montes, nascetur ridiculus mus.
Nulla consequat massa quis enim. Donec pede justo, fringilla vel, aliquet nec, vulputate eget, arcu. In enim justo, rhoncus ut, imperdiet a, venenatis vitae, justo. Nullam dictum felis eu pede mollis pretium.
Routine Care to Complete Smile Transformations
Whether you need a complete smile transformation with full mouth implants, dentures or caring family dentistry, Dr. Wright and his team deliver exceptional results with a personal touch.
Smile Transformations
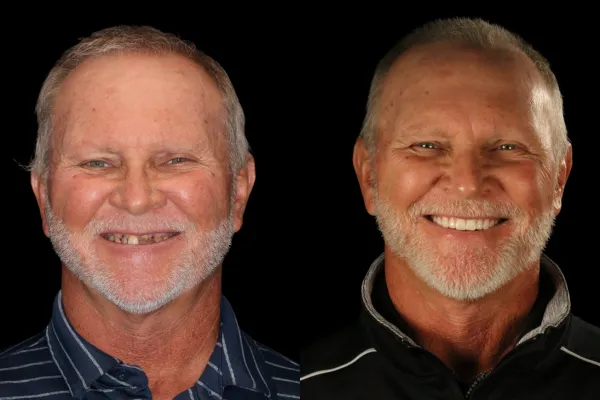
If you are looking for a new smile transformation with dental implants, dentures or other cosmetic options, we'll create a personalized plan to give you the confident, beautiful smile you deserve. Dr. Wright is one of the nation's top-rated dental implant specialists who specializes in smile transformations and has transformed more than 3,000 smiles with precision, artistry, and care.
General Dentistry

Our team provides compassionate, comprehensive care for your whole family. As your trusted dentist in Corsicana, we treat you like family, not a number, and take the time to make every visit comfortable and stress-free for every patient no matter how young, or young at heart.
Emergency Dental

Dental emergencies don't wait, and neither do we. Whether it's a cracked tooth, severe pain, or a knocked-out tooth we're here to help fast. Same-day appointments available in most cases.
Meet Our Team
Where Comfort, Compassion, and Expertise Come Together

Personal care you can trust.
You'll be surprised how different it feels here. Many of our patients drive over an hour, some even fly in from across Texas and out of state, because they know they'll receive high quality dental implants and care that's truly exceptional.
Our Blogs
Take the First Step!
Your journey starts with one simple conversation.
Our Smile Coordinator will:
Listen to your goals & concerns
Evaluate your oral health
Discuss personalized treatment options
Explain costs, financing and insurance options – no pressure
Simply fill out the form and our Smile Coordinator will reach out to you soon!
Ready to talk now?
Call or text us today!
903-872-8422

Our Service Areas
Just Wright Dental and Implant Center proudly serves patients across Navarro County and the greater Dallas–Fort Worth area. Click your city to learn more about dental care near you.
Follow Us
Follow Us
Serving Navarro County and the greater Dallas–Fort Worth area with gentle, smile transformation, dental iimplants, denture and family-focused dental care.
Dental Care
More
Contact Us
903-872-8422
1430 W 2nd Ave, Corsicana, TX 75110
- Monday - Friday, 8:00 am - 5:00 pm
© Copyright 2026. Just Wright Dental and Implant Center. All rights reserved.